
Reciprocal Development: Dismantling Urban Power Monopoly
Part 3 of the Rural Health Equity Framework™ series

Over the last fortnight I explored Rural-First Design and Function-Led Delivery - the first two components of the Rural Health Equity Framework. This week, I’m unpacking the third: Reciprocal Development.
When the Language Reveals the Power
Notice the language we use about rural health development:
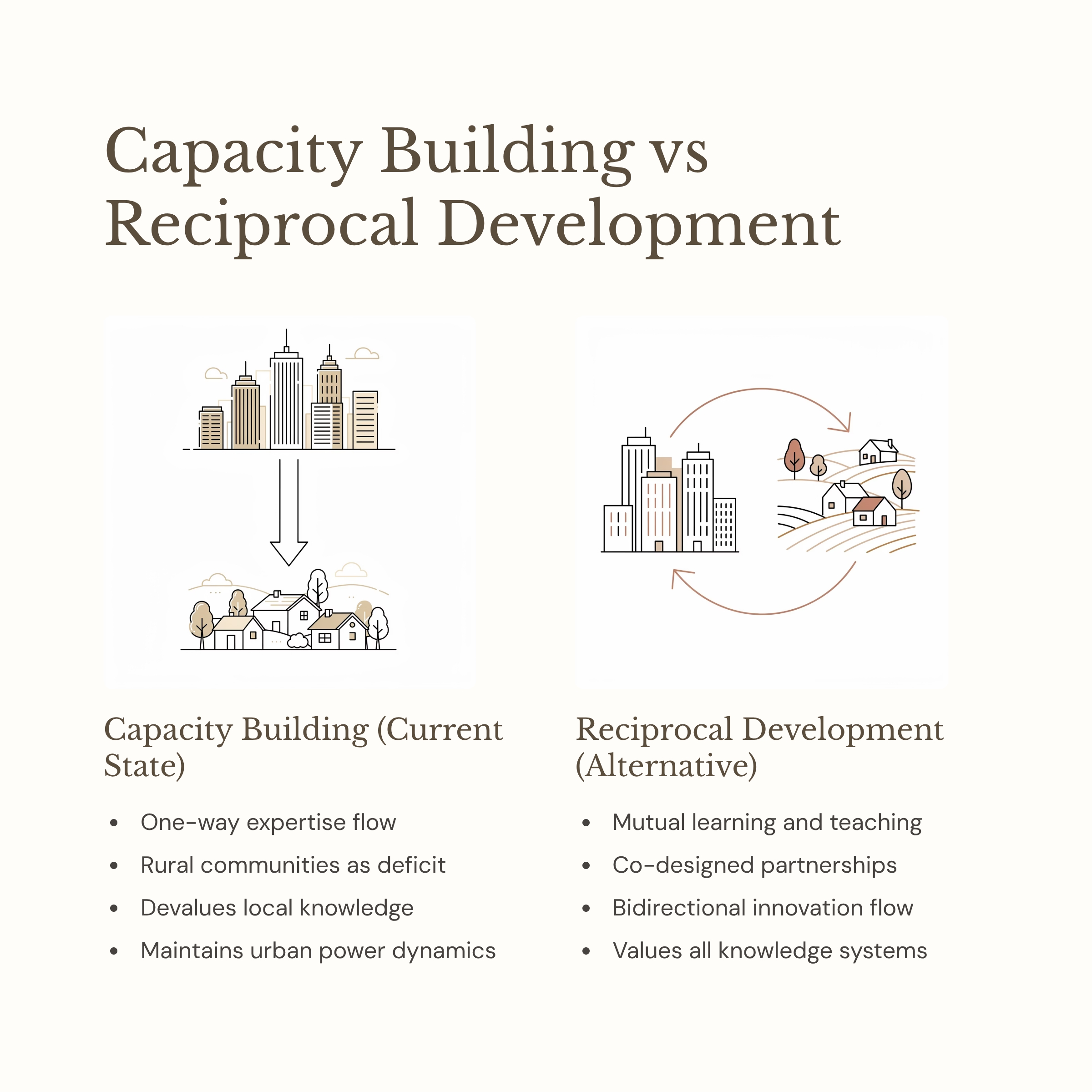
“Building capacity” in rural areas. “Upskilling” rural practitioners. Urban experts travelling rural to “teach.” Professional development “delivered” to rural communities. Research done ON rural populations.
This language speaks volumes.
It positions urban as expert and rural as perpetually needing help. It assumes knowledge flows one direction. It frames rural as deficit rather than different.
During COVID lockdowns, I watched this play out in real time. Our rural practitioners were innovating rapidly - finding creative solutions to maintain care for their communities when usual systems collapsed. We were problem-solving, adapting, doing what rural health professionals have always done.
And then our urban colleagues stepped in to “govern” what we were doing. Calling halts to activity without being prepared to understand the consequences. The automatic assumption that innovation needed oversight from the centre, that rural couldn’t be trusted to problem-solve.
It’s like an urban power monopoly; this assumption that cities know best and rural needs capacity building.
What Reciprocal Development Actually Means
Reciprocal Development is the third component of my Rural Health Equity Framework. It dismantles urban power monopoly and builds toward something fundamentally different: tuakana-teina relationships.
For my international readers: tuakana-teina is a learning relationship from te ao Māori (the Māori world). Tuakana (older or more experienced) and teina (younger or less experienced) work together, but the relationship is reciprocal. Both teach, both learn. The roles shift depending on context and expertise. It’s not hierarchical mentorship, it’s mutual support where everyone has mana (authority, prestige, integrity).
In health systems, this means:
Rural and urban practitioners as equals with different expertise
Bidirectional innovation exchange
Co-designed professional development
Research as partnership, not extraction
Urban learning FROM rural, not just teaching TO rural
The barrier being dismantled: One-way knowledge transfer that assumes expertise only flows from cities outward.
The inclusive alternative: Mutual teaching and learning where both rural and urban bring expertise the other needs.
Keep reading with a 7-day free trial
Subscribe to Allied - Insights for a Thriving Rural Workforce to keep reading this post and get 7 days of free access to the full post archives.